康德診所
最新消息
診所介紹
康德診所是一間以慢性病與中年族群健康管理為核心的診所
康德診所榮獲108-113年「中央健康保險署糖尿病品質支付服務方案」品質卓越獎
康德診所獲選康健雜誌身體百科糖尿病100問專刊:全台最佳糖尿病照護醫院診所之一
獲得獎項
診所設備
診所檢驗項目
康德診所主治項目
服務項目
內科疾病
糖尿病共同照護網
高血壓
高血脂
痛風
初期慢性腎臟病照護網
腸胃疾病
B型肝炎C型肝炎個案追蹤
甲狀腺疾病
脂肪肝 慢性肝炎
氣喘共照網
慢性肺阻塞照護
失眠憂鬱焦慮
失眠
憂鬱症
焦慮
泌尿系統疾病
腎結石
泌尿道感染
攝護腺肥大
成人預防保健
國健局免費成人健康檢查
國健署大腸癌糞便潛血篩檢
國健署免費口腔黏膜篩檢
公司工廠學校健檢報告諮詢、複檢追蹤
門診戒菸
預防接種
子宮頸癌疫苗
麻疹德國麻疹腮腺炎疫苗
白喉百日咳破傷風補追加疫苗
自費B型肝炎疫苗
A型肝炎疫苗
四價流感疫苗
水痘疫苗
帶狀皰疹疫苗
門診時間
康德診所114年1月1日起門診時間表
營養師衛教時段
專業人員
蕭秀娟營養師
高英哲醫師
王宣惠醫師
林嘉貞醫師
李佩娟醫師
許冬穎營養師
衛教文章
內科疾病
糖尿病
高血壓
高血脂
胸腔疾病
腎臟疾病
氣喘專區
皮膚病
腸胃疾病
泌尿道疾病
預防保健
飲食衛教
減重相關
運動相關
預防注射
健康食品
心理健康
老人醫學
旅遊醫學
首頁
服務項目
服務項目
服務項目
全部服務項目
請選擇排序方式
上架時間 新→舊
上架時間 舊→新
每頁顯示12筆
每頁顯示16筆
每頁顯示20筆
每頁顯示24筆
one
two
four
代謝症候群照護
代謝症候群是一組可預防且可改善的健康問題,包括腹部肥胖、高血壓、高血糖、高血脂等指標。如果這些指標同時出現在你身上,就可能增加未來 糖尿病、心血管疾病、中風 等慢性病的風險。預防比...
DETAIL
公司工廠學校健檢報告諮詢、複檢追蹤
遇到健檢報告異常可以攜帶報告來康德診所由專業的家庭醫學專科醫師、職業醫學專科醫師判讀報告並視需要安排進一步複檢。
康德診所有齊全的儀器、血液、尿液、生化、心電圖、肺功能、視力檢查...
DETAIL
糖尿病共同照護網
唯有醫師偕同護理師、營養師,幫助患者改變徹底改變生活習慣才能戰勝糖尿病。
DETAIL
高血壓
周全的高血壓評估與齊全的治療藥物
DETAIL
高血脂
DETAIL
痛風
痛風發作時期給予症狀控制,平時藉由飲食控制與降尿酸藥物避免痛風再次發作,並發現腎結石、痛風石等併發症。
DETAIL
氣喘共同照護網
咳不停嗎?正確診斷氣喘,解決你的問題
DETAIL
初期慢性腎臟病照護網
保護腎臟,幫助病人控制好血壓、血脂、尿酸,避免腎衰竭。
DETAIL
健保署B型肝炎、C型肝炎個案追蹤計畫
B型肝炎、C型肝炎帶原者應每3-6個月進行追蹤檢查,包含血液檢查與腹部超音波。
DETAIL
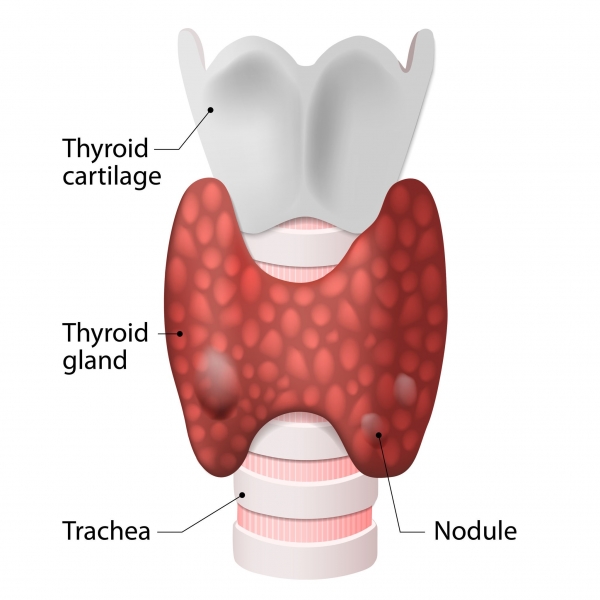
甲狀腺疾病
甲狀腺機能亢進、甲狀腺機能低下、甲狀腺結節、藥物治療、超音波檢查、血液檢查。
DETAIL
慢性肺阻塞照護
肺阻塞需要長期治療,所以康德診所有加入健保署的肺阻塞照護計畫。每次回診時肺功能檢查可以幫助醫師確認患者疾病的嚴重程度。
為了照顧社區肺阻塞的患者讓患者免於在醫院間奔波,我們有齊全...
DETAIL
腸胃疾病
腹痛 胃潰瘍 胃食道逆流 大腸激躁症 膽結石 膽囊息肉
DETAIL
<
1
2
3
>
1
2
3
TOP
繁體中文
最新消息
診所介紹
康德診所是一間以慢性病與中年族群健康管理為核心的診所
康德診所榮獲108-113年「中央健康保險署糖尿病品質支付服務方案」品質卓越獎
康德診所獲選康健雜誌身體百科糖尿病100問專刊:全台最佳糖尿病照護醫院診所之一
獲得獎項
診所設備
診所檢驗項目
康德診所主治項目
服務項目
內科疾病
糖尿病共同照護網
高血壓
高血脂
痛風
初期慢性腎臟病照護網
腸胃疾病
B型肝炎C型肝炎個案追蹤
甲狀腺疾病
脂肪肝 慢性肝炎
氣喘共照網
慢性肺阻塞照護
失眠憂鬱焦慮
失眠
憂鬱症
焦慮
泌尿系統疾病
腎結石
泌尿道感染
攝護腺肥大
成人預防保健
國健局免費成人健康檢查
國健署大腸癌糞便潛血篩檢
國健署免費口腔黏膜篩檢
公司工廠學校健檢報告諮詢、複檢追蹤
門診戒菸
預防接種
子宮頸癌疫苗
麻疹德國麻疹腮腺炎疫苗
白喉百日咳破傷風補追加疫苗
自費B型肝炎疫苗
A型肝炎疫苗
四價流感疫苗
水痘疫苗
帶狀皰疹疫苗
門診時間
康德診所114年1月1日起門診時間表
營養師衛教時段
專業人員
蕭秀娟營養師
高英哲醫師
王宣惠醫師
林嘉貞醫師
李佩娟醫師
許冬穎營養師
衛教文章
內科疾病
糖尿病
高血壓
高血脂
胸腔疾病
腎臟疾病
氣喘專區
皮膚病
腸胃疾病
泌尿道疾病
預防保健
飲食衛教
減重相關
運動相關
預防注射
健康食品
心理健康
老人醫學
旅遊醫學